869
Views & Citations10
Likes & Shares
Helicobacter pylori colonize the human gastric
epithelium, causing chronic gastritis, peptic ulcer disease and gastric cancer.
This work determined the level of IgG seropositivity to Helicobacter pylori in peptic ulcerative individuals. A cross
sectional study involving 179 peptic ulcerative individuals was conducted.
Ethical approval was obtained and informed consent sought. Questionnaire was
administered and 5 ml of blood was collected into EDTA containers. Subject
selection was done using convenience sampling technique. The H. pylori seropositivity was determined
using ELISA technique. The prevalence rate for H. pylori was 51.4% and the predominant seropositive age group was
24-35 years (22.9%). Age (p=0.00) was found to be a significant risk factor for
H. pylori seropositivity. Females 50 (27.9%) were more seropositive to H. pylori than males 42 (23.5%) though the difference was not
significant (p=0.281). Moreover, there was no significant relationship between
source of drinking water and H. pylori
seropositivity (p=0.433). Overall, borehole water 16 (8.9%) and sachet water
consumers 57 (31.8%) predominated in the seropositive population. The results show that H. pylori
is high among peptic ulcerative individuals in Nnewi and also, increased levels
of interferon gamma may contribute to the development of H. pylori associated diseases.
Keywords: Helicobacter pylori, Peptic, Risk factors, Seropositivity, Prevalence, Interferon gamma
Helicobacter pylori (H.
pylori) infection
is the most common chronic bacterial infection around the world [1]. It has
been shown that 50% of adults in developed countries and 90% of adults in
developing countries were positive of serum antibodies against H. pylori [2]. The critical period at which H.
pylori is acquired, is during childhood, especially in the developing
countries and areas of overcrowding and socioeconomic deprivation [3]. This
bacterium is a small spiral Gram-negative organism. Factors important for
colonization include motility, environmental sensing, chemotaxis [4], iron
acquisition [5] and acid resistance. The pathogen is the main cause of peptic
ulceration, gastric adenocarcinoma, and gastric mucosa-associated lymphoid tissue (MALT) lymphoma [6]. It
is considered that H. pylori infection is the most common cause of
morbidity and mortality in upper digestive tract diseases. Currently, the
effects of H. pylori infection on the development of extra alimentary
ailments such as coronary disease, myocardial infarction, idiopathic
thrombocytic purpura, iron deficiency anemia has been shown [7]. However, only
10-15% of those colonized develop disease while 85-90% remains asymptomatic and
pathogenesis depends upon strain virulence, host genetic susceptibility and
environmental cofactors. Virulence factors include the cytotoxin-associated
gene (cag) pathogenicity island (PAI), which induces pro-inflammatory,
pro-proliferative epithelial cell signaling; the cytotoxin VacA, which causes
epithelial damage; and blood group antigen binding adhesin (BabA). Host genetic
polymorphisms that lead to high-level pro-inflammatory cytokine release in
response to infection increase cancer risk.
The relation between H. pylori infection and lifestyle is uncertain, but its intensification in the individual populations is strongly related to economic conditions [2]. Developing countries are at highest risk, due to people living in poor socioeconomic conditions. The increasing risk factor includes; poor sanitary conditions, overpopulation, street stalls and unsafe water supply sources [8]. Epidemiological studies demonstrate that the incidence of H. pylori infection appears to be higher in children than in adults, possibly due to lower standards of personal hygiene in younger populations [3,9]. Human is the main reservoir of this infection [2,10]. Infected mother and older siblings are important factors for H. pylori transmission to children. The transmission routes are oral-oral (by saliva), which prevails in the developed world, fecal-oral (person-to-person or by contaminated water, or maybe food), mainly in the developing countries or gastro-oral (by vomiting and regurgitation).
Methods available for diagnosis
of H. pylori include: Invasive Methods such as Endoscopic diagnosis,
microscopic examination of histological sections, culture of biopsy specimen,
molecular detection of H. pylori
using Polymerase Chain Reaction (PCR), Rapid Urease Test. Non-Invasive method
such as Urea Breath test, Antibody test using either Enzyme Linked
Immunosorbent Assay (ELISA) technique or Immunochromatography Test (ICT)
technique, H. pylori stool antigen
test [11].
MATERIALS AND
METHODS
Study design
A cross
sectional study was conducted among 184 peptic ulcerative individual selected
from the medical outpatient clinic and internal medicine clinic of Nnamdi
Azikiwe university (NAUTH), Nnewi using convenience sampling technique. Ethical
approval (with approval number: NAUTH/CS/66/VOL8/31) was obtained from the
ethics committee of NAUTH. The participants were diagnosed of peptic ulcer by
the physician. Informed consent was obtained from the participants.
Study population
Subjects
included in the study were aged from 15-70 years, having persistent or
recurrent abdominal pain or discomfort and with at least two of the symptoms of
the epigastric pain and associated symptoms such as bloating, nausea,
flatulence and anorexia. All subjects that are pregnant, outside the age of
15-70, currently on antibiotics treatment and do not present with any sign of
peptic ulcer were excluded. Questionnaires include data on participant’s
demography, symptoms of peptic ulcer, preferred eating habits, source of
drinking water and antibiotics use.
Sample collection
Five (5)
milliliters of blood was drawn from the participants using 5 ml syringe and was
dispensed into a plain container. The serum was separated and stored at -20°C
for Enzyme Linked Immunosorbent Assay (ELISA) H. pylori assay. Assay for H.
pylori IgG antibodies in patients sample was according to the
manufacturer’s instructions. The ELISA test was performed using Mindray ELISA
machine (Shenzhen, China) and the H.
pylori IgG ELISA kit by Biochem incorporated (Canada).
Purified H.
pylori antigen was coated on the surface of micro wells. Diluted patients
serum was added to the wells and the H. pylori
IgG-specific antibody, if present, binds to the antigen. All unbound materials
were washed away. Enzyme conjugate was added, which binds to the
antigen-antibody complex. Excess enzyme conjugate was washed off and substrate
and chromogen added. The enzyme conjugate catalytic reaction was stopped at a
specific time. The intensity of the color generated was proportional to the
amount of IgG-specific antibody in the sample. The results were read using a
micro well reader compared in a parallel manner with calibrator and controls [12].
STATISTICAL ANALYSIS
The data was
statistically analyzed using SPSS version 20. Values were expressed as mean ±
standard mean error. The student's t-test and chi square were used and
considered significant if p-value˂0.05.
RESULTS
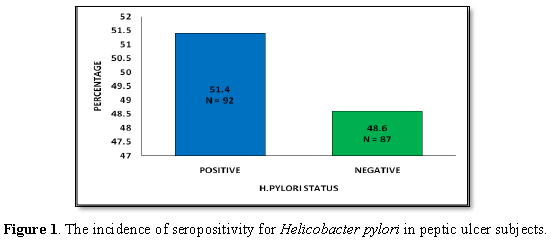
The IgG seropositivity for H. pylori infection was positive in 92
and negative in 87 subjects, 5 participants had indeterminate results and were
not included in the study population. Figure
1 shows the incidence of seropositivity for Helicobacter pylori in peptic ulcerative subjects. Results indicate
that a greater percentage (51.4%) of subjects tested positive for H. pylori. On the other hand, 48.6%
tested negative for H. pylori.
However, no statistical difference (p=0.709) was observed between the
seropositivity and seronegativity for H.
pylori.
Table 1 shows the
frequency distribution of subjects according to their age groups and Helicobacter pylori statuses. Data
indicate that age group “25-34 years” had the greatest percentage, 44.6% (n=41)
of seropositive subjects, followed by subjects aged 35-44 years, 17.4% (n=16).
Age group ≥ 65 years had the least percentage of seropositivity. Seronegativity
was greatest (29.9%) in age group 35-44 years and lowest (2.3%) in age group
25.34 years. Chi-square test (χ2=51.87) shows significant
association (p<0.001) between age and H.
pylori status of subjects.
Table 2 reveals the frequency
distribution of subjects according to their sex and Helicobacter pylori status. Results indicate that a greater
percentage of females tested both positive (54.3%) and negative (59.8%) for H. pylori than the males (positive,
45.7% and negative, 40.2%). Chi-square test (χ2=0.536) indicated no
significant association (p=0.281) between sex and H. pylori status of subjects.
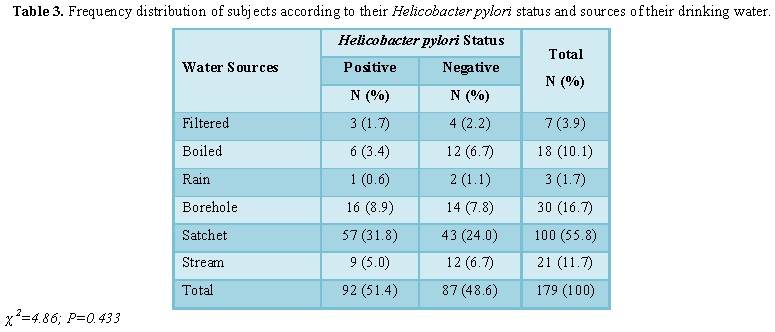
Table 3 shows the
frequency distribution of subjects according to their Helicobacter pylori status and sources of their drinking water.
Results indicate that majority, (57 (62%)) of the seropositive subjects were
those who drink ‘sachet’ water, followed by those who consume borehole water
(16 (17.4)). Subjects who drink rain water had the least percentage (1.1%) of
seropositivity for H. pylori.
Subjects who use ‘sachet’ water also had the highest percentage (49.4%), while
those who use rain water also had the least percentage (2.3%) of seronegativity
for H. pylori. Chi-square test (χ2=4.86)
indicated no significant association (p=0.433) between source of water and H. pylori status of subjects.
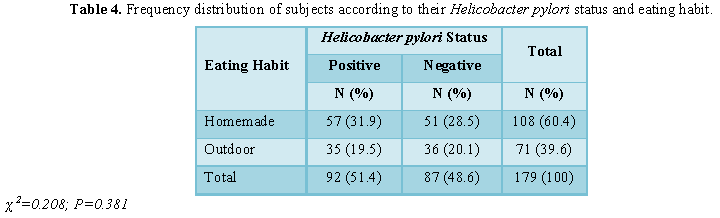
Table 4 shows the frequency distribution of subjects according to their Helicobacter pylori status and eating
habit. Data show that those who eat homemade foods had greater percentage (62%)
of seropositivity compared to those who eat outdoor (38%). The same trend was
also observed in incidence of seronegativity status of subjects (homemade,
58.6%; outdoor, 41.4%). Chi-square test (χ2=0.208) indicated no
significant association (p=0.381) between eating habit and H. pylori status of subjects.
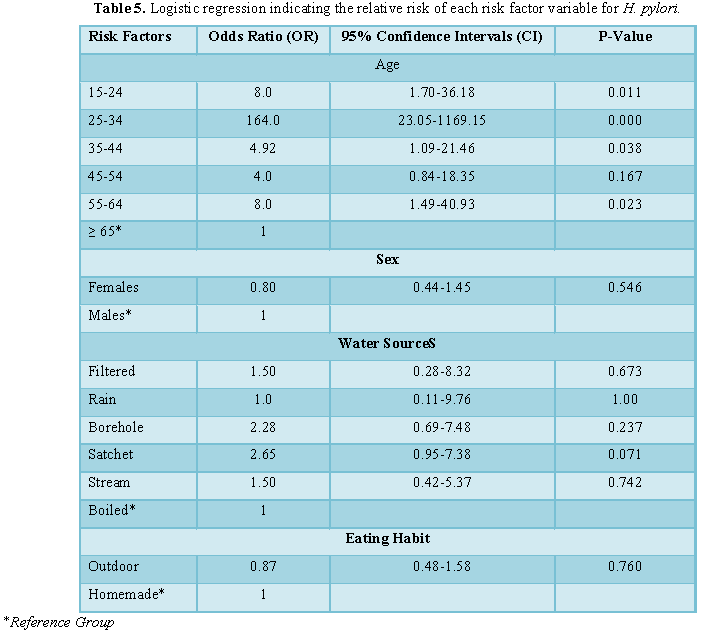
Table 5 shows the logistic
regression test indicating the relative risk of each risk factor variable for H. pylori. Results indicate that the
risk of testing positive for H. pylori
is significantly greater in subjects aged 15-24 years (OR=8.0; p 0.011), 25-34
years (OR=164; p=0.006), 35-44 (OR=4.9; p=0.038) and 55-64 years (OR=8.0;
p=0.023) compared to those aged ≥ 65 years. In contrast those aged 45-54 years
did not indicate significantly greater risk compared to those aged ≥ 65 years.
The females did not indicate significantly (p=0.546) greater risk for H. pylori seropositivity compared to
the males. Similarly, no significant greater risk of H. pylori were observed in those who make use of filtered
(p=0.673), rain (p=1.0), borehole (p=0.237), sachet (p=0.07) and stream
(p=0.742) water sources compared to those who use ‘boiled’ water. Furthermore,
subjects who eat outdoor did not indicate significantly (p=0.760) greater risk
for H. pylori seropositivity compared
to those who eat homemade foods.
DISCUSSION
The results from this
study show that the seroprevalence rate of H.
pylori in the study population is 51.4%. This is similar to the 58.3%
obtained by Abiodun et al. [13] in Ibadan among peptic ulcerative patients and
also similar to the 58% obtained by Obiajuru et al. [14] in Orlu, Imo state
among duodenal and gastric ulcer patients. Similarly, Tijjani and Umar [15] found
a prevalence of 93.3% among peptic ulcerative patients in Kano [16], in their epidemiological
study in south east Nigeria, reported a prevalence of 51.75% among those living
in high densely populated environment, exposed to fecal contaminated water,
poor hygiene and low level of education and 17.66% among those living in low
density populated areas. In Kaduna, Nwodo et al. [17] obtained a
seroprevalence rate of 80.4% while Olokoba et al. [18] got a seroprevalence of
93.6% among dyspeptic patients that underwent gastroscopy in Maiduguri.
Though the prevalence
rate obtained in this study is high, when compared to earlier studies carried
out in the Northern part of the country, it is much lower but the values gotten
from the eastern and western part of the country are similar to that gotten in
this study. This lower prevalence could reflect the comparatively higher
standards of hygiene among South eastern and South western Nigerians compare to
that of Northern Nigerians, since H. pylori
prevalence is higher among those living in high densely populated environment, exposed to fecal
contaminated water, poor hygiene and low
level of education compare to that of low density populated areas [16]. These
findings show that H. pylori is
implicated in most peptic ulcer diseases. Studies have shown that use of
non-steroidal anti-inflammatory drugs (NSAID) is the major cause of H. pylori negative peptic ulcer [19]. The seropositivity
level increased from 15-24years (8.4%) and peaked at 25-34 years (22.9%) and
then declined to 1.1% at greater than 65 years. It was statistically
significance with P=0.000 showing that age is a risk factor for H. pylori. The H. pylori prevalence according to different age group as seen in
this study is in accordance with what was obtained in other studies, where
prevalence of H. pylori increased at
earlier age, then declined in population over 60 years in Pakistan, France and
over 50 years in other countries like Vietnam, Algeria and Ivory Coast [20]. In
contrast, some studies claimed that Helicobacter
pylori prevalence increased with age [21].
H. pylori infection is acquired at younger age [3]. In this study
also H. pylori seropositivity could
be seen to be high in younger population which suggests that the infection was
acquired during childhood and early adolescent, reaching its peak at adulthood.
This observation is in concordance with findings of Jaff [22]. On the other
hand, out of 18 peptic ulcer subjects that fall within the age bracket of 65
years and above, 2 (1.1%) were seropositive to H. pylori while 16 (8.9%) were seronegative to H. pylori. Most studies stated that stomach ulcers are more likely
to develop in older people [23]. This is because arthritis is prevented by
daily use of aspirin and NSAIDs, in addition to age related, relaxation of
pylorus valve which allows backflow of bile to erode the stomach lining [23].
Also, Ananya et al. [24] opined that because prostaglandin levels in the
gastric mucosa are decreased in elderly patients, ageing are associated with
diminished epithelial cell turnover rate and a reduced capacity to repair the
gastric mucosa. In this study, there were more females 102 (57%) than males 77 (43%);
it was observed that H. pylori
prevalence was more in females. Out of the 92 (51.4%) patients that were
seropositive, 50 (27.9%) were female and 42 (23.5%) were male. It was observed
that H. pylori seropositivity has no
significance with sex (P=0.281) which shows that sex is not a risk factor.
There are varying reports of higher prevalence of H. pylori infection in either male or female, but with no
significant association between the infectivity rate and sex [25,26].
Moreover, Ezugwu and
Chibuike [16] stated that lifestyle play a major role in H. pylori infection, also they observed that source of water supply
used by the participant had an effect on the transmission of infection. Most of
their study group used stream water, well water which could be fecally
contaminated and few used tap water and bottled water. In this study, though
there was no association between source of water and H. pylori (P=0.433) but majority of the participants that are H. pylori positive consume sachet water
and borehole water which could be contaminated as a result of improper
processing of the sachet water, contamination by water vendors or inadequate
drilling of the boreholes. Also eating habit (P=0.381) did not prove to be a
risk factor in this study. This is consistent with the findings of Valliani et
al. [27].
CONCLUSION
Helicobacter pylori are major cause of peptic ulcer in humans. This
work has shown that the prevalence of H.
pylori seropositivity is high in the study environment but lower than what
is obtained in northern Nigeria. H.
pylori seropositivity is found to be significantly related to the age of
the individual. In addition, the ABO blood group of the individual was also
found to be a significant factor in H.
pylori seropositivity and blood group A are of greater risk. Moreover,
seropositivity was found to increase with age of the subjects, so older adults
are at more risk of infection. Since majority of those infected either consumed
borehole or sachet water, it suggests that most of the boreholes might be
contaminated and that the sachet water might not be well processed. In addition
even when the sachet water was well processed, people could be infected by the
activities and unhygienic attitude of some water vendors. Interferon gamma
levels were also found to be higher among those seropositive for H. pylori compared to the H. pylori seronegative individuals. The
gamma interferon contributes to the H.
pylori associated inflammation which leads to gastric and intestinal
ulceration.
CONFLICT OF INTEREST
The authors
declare that there are no conflicts of interests
AUTHOR’S CONTRIBUTION
C.O.M., C.G.O.
J.Z.A, designed research, C.G.O, C.O.M. M.P.O, performed research, A.J.C,
M.P.O. analysed data, C.G.O., C.O.M, J.Z.A. wrote paper.
1.
Kanbay M, Gur G, Arslan H (2005) The relationship
of ABO blood group, age, gender, smoking and Helicobacter pylori
infection. Digest Dis Sci 50: 1214-1217.
2.
Fozieh JM, Tahereh N, Mansour A (2014)
Antibacterial activity of garlic (Allium sativum) on multidrug
resistance Helicobacter pylori isolated from gastric biopsies. Int J
Enteric Pathog 2: 16749.
3.
Moayyedi P, Axon AT, Feltbolwer R (2002) Relation
of adult lifestyle and socioeconomic factors to the prevalence of Helicobacter
pylori infection. Int J Epidemiol 31: 624-631.
4.
Terry K, Williams SM, Connolly L, Ottemann KM (2005)
Chemotaxis plays multiple roles during Helicobacter pylori animal
infection. Infect Immuunity 73: 803-811.
5.
Waidner B, Greiner S, Odenbreit S, Kavermann H,
Velayudhan J (2002) Essential role of ferritin Pfr in Helicobacter
pylori iron metabolism and gastric colonization. Infect Immununity 70:
3923-3929.
6.
Jing C,
Huang ZJ, Duan YQ (2012) Glulathione-s-transferases gene polymorphism in
prediction of gastric cancer risk by smoking and Helicobacter pylori
infection status. Asian Pac J Cancer Prev 13: 3325-3328.
7.
Celinski K, Kurzeja-Miroslaw A, Slomka M (2006) The
effects of environmental factors on the prevalence of Helicobacter pylori
infection in inhabitants of Lublin Province. Ann Agric Environ Med 13: 185-191.
8.
Zhong C, Li NK, Bi JW (2012) Sodium intake, salt
taste and gastric cancer risk according to Helicobacter pylori
infection, smoking, histological type and tumor site in China. Asian Pac J
Cancer Prev 13: 2481-2484.
9.
Ofonime M, Enobong EI, Emmanuel EE (2012)
Seroepidemiology of Helicobacter pylori infection among children seen in
a tertiary hospital in Uyo, southern Nigeria. Pan Afr Med J 12: 39.
10.
Lyudmila B (2015) Epidemiology of Helicobacter
pylori infection. Horizon Scientific Press, p: 278. Available at: http://www.horizonpress.com/helicobacter
11.
Megraud F, Bessede E, Lehours P (2014) Diagnosis of
Helicobacter pylori infection. Helicobacter 19: 6-10.
12.
Ochei J,
Kolhatkar A (2000) Medical laboratory science theory and practice. 7th
Edn. Tata McGraw-Hill Publishing Company Limited, pp: 356-1174.
13.
Abiodun CJ,
Jesse AO, Samuel OO, Olayiwola AO, Adegboyega A (2010) Prevalence of Helicobacter
pylori among Nigerian patients with dyspepsia in Ibadan. Pan Afr Med J 6:
18.
14.
Obiajuru IOC, Adogu POU (2013) Prevalence of Helicobacter
pylori and other intestinal parasites amongst duodenal and gastric ulcer
patients at Imo state University Teaching Hospital, Orlu, south-eastern
Nigeria. J Med Med Sci 4: 362-369.
15.
Tijjani B, Umar A (2008) Peptic ulcer disease and Helicobacter
pylori infection at Kano, Nigeria. Internet J Gastroenterol 8: 1.
16.
Ezugwu RI, Chibuike C (2014) Epidemiology of Helicobacter
pylori infection among dyspepsia patients in south-east, Nigeria. J Pharm
Biol Sci 9: 53-56.
17.
Nwodo EN, Yakubu SE, Jatau ED, Yabaya A (2009)
Seroprevalence of Helicobacter pylori infection in patients with
gastritis and peptic ulcer disease in Kaduna, Kaduna state, Nigeria. Afr J
Basic Appl Sci 1: 123-128.
18.
Olokoba AB, Gashau W, Adamu A, Salawu FK (2013) Helicobacter
pylori infection in Nigeria with dyspepsia. Ghana Med J 47: 79-81.
19.
Atherton JC, Blaser MJ (2004) Helicobacter
pylori infections. In: Harrison’s Principals of Internal Medicine, ed.
Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JL. 16th
Edn. New York: McGraw-Hill, pp: 886-889.
20.
Ozaydin N, Turkyilmaz SA, Cali S (2013) Prevalence
and risk factors of Helicobacter pylori in Turkey: A
nationally-representative, cross-sectional, screening with the13C-Urea breath
test. Biometric Central Public Health 13: 1215.
21.
Parente F, Cucino C, Bianchi PG (2003) Treatment
options for patients with Helicobacter pylori infection resistant to one
or more eradication attempts. Digest Liver Dis 35: 523-528.
22.
Jaff MS (2011) Relation between ABO blood groups
and Helicobacter pylori infection in symptomatic patients. Clin Exp
Gastroenterol 4: 221-226.
23.
Seyda T, Derya C, FüsunA, Meliha K (2007) The
relationship of Helicobacter pylori positivity with age, sex and ABO/Rhesus
blood groups in patients with gastrointestinal complaints in Turkey.
Helicobacter 12: 244-250.
24.
Ananya C, Sirshendu C, Sandip KB (2012) H.
pylori induced gastric ulcer: Pathophysiology and herbal remedy. Int J Biol
Med Res 3: 1461-1465.
25.
Lesi OA, Kehinde MO (2003) Prevalence of Helicobacter
pylori antibodies and predominant symptom complex of patients with
dyspepsia. J Clin Sci 3: 7-11.
26.
Smith SI, Oyedeji KS, Arigbabu AO, Chibututu CC,
Atimomo CE, et al. (2001) Seroprevalence of Helicobacter pylori infection
in patients with gastritis and peptic ulcer in western Nigeria. Br J Biomed Sci
58: 97-100.
27.
Valliani A, Khan F, Ahmed B (2013) Factors
associated with Helicobacter pylori infection, results from a developing
country, Pakistan. Asian Pac J Cancer Prev 14: 53-56.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5


QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Journal of Pathology and Toxicology Research
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)


